CASE REPORT |
https://doi.org/10.5005/jp-journals-10019-1366 |
Smile Makeover Utilizing Digital Esthetic Veneers Workflow: A Case Report
1Department of Restorative Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia
2Department of Prosthodontics, Ministry of Health (MOH), Saudi Arabia; Department of Prosthodontics, Faculty of Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia
Corresponding Author: Walaa Magdy Ahmed, Department of Restorative Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia, Phone: +9660505562836, e-mail: wmahmed@kau.edu.sa
Received on: 15 September 2022; Accepted on: 25 November 2022; Published on: 30 March 2023
ABSTRACT
This case report describes an innovative approach to creating a smile makeover using a fully digital workflow. An intraoral scan was integrated into the patient’s frontal smile using digital software to create a three-dimensional (3D) digital smile design and virtual mock-up, guided by universal esthetic analysis principles. The virtual mock-up was 3D printed to fabricate an index for the clinical mock-up. The clinical mock-up was applied using acrylic materials to translate the virtual mock-up clinically and obtain patient consent. Esthetic analyses were performed to obtain optimum esthetic, functional, and occlusal stabilities. Guided to veneer preparations were performed. Retraction cords were placed, and an intraoral scan was performed for the #15 and #25 veneers. The margin was defined digitally, and the stereolithography (STL) files were then transferred digitally to the laboratory technician for veneer fabrication. Provisional veneers were cemented using the spot-etch technique. Computer-aided design and computer-aided manufacturing (CAD/CAM) lithium disilicate veneers were bonded to the prepared teeth. Esthetic function and occlusion remained stable at the 1-year follow-up visit. The use of digital workflow in managing esthetic cases enhanced the treatment predictability and increased the survival and success of the restorations due to the conservation of tooth structure.
How to cite this article: Ahmed WM, Althagafi RA. Smile Makeover Utilizing Digital Esthetic Veneers Workflow: A Case Report. Int J Prosthodont Restor Dent 2022;12(3):145-148.
Source of support: Nil
Conflict of interest: None
Patient consent statement: The author(s) have obtained written informed consent from the patient for publication of the case report details and related images.
Keywords: Guided tooth preparation, Three-dimensional digital smile design, 3D printing, Virtual mock-up.
BACKGROUND
Nowadays, modern societies are seeking attractive smiles to elevate their self-image and improve their level of acceptance in their professional careers. Esthetic veneers are a highly requested treatment by patients and are not only limited to actresses and celebrities. This went beyond them to individuals in the general population. The ability of ceramic veneers to control the reduction of tooth structure in a precise and measurable way during tooth preparation is a clinical challenge.1
Digital tools offer a new perspective on daily clinical activities. Digital information serves as a starting point for intraoral mock-ups, which are widely reported in the literature as an objective and efficient communication tool among dentists, patients, and technicians.2-11 Moreover, intraoral scanners showed comparable and sometimes higher accuracy in precision and trueness compared to conventional polyvinyl siloxane (PVS) impressions in partial and full arch cases.12,13
With advancements in digital technology, it is now possible to perform a diagnostic setup for maxillary and mandibular teeth in a timely manner and to utilize these digital setups to guide tooth preparation and crown lengthening procedures, and cementation guides.1,14,15
This article aims to describe an approach to creating a smile makeover using a fully digital veneer workflow to fabricate 3D printed smile design models that can be translated into the clinical setting for veneer preparation and provisionalization. The preparation was then recorded accurately using an intraoral scanner and digitally submitted to a laboratory technician for veneer production.
CASE DESCRIPTION
A 40-year-old patient with nonsignificant medical conditions (a patient with mild systemic disease) visited a private clinic seeking to create a new smile to enhance his stained and esthetically unproportional teeth. He smokes 2–3 packets of cigarettes per day. He had a history of prepless veneers with bulky restorations and requested removal 2 weeks after bonding.
Extraoral examination revealed an asymmetrical facial proportion vertically, with the nose deviating to the right (Fig. 1A). Intraoral examination revealed heavily stained teeth (Figs 1B to G). Orthodontic treatment was recommended for the patient to correct the curve of Spee prior to performing veneers preparation and cementation to reduce the amount of tooth structure removal. However, the patient rejected this option.
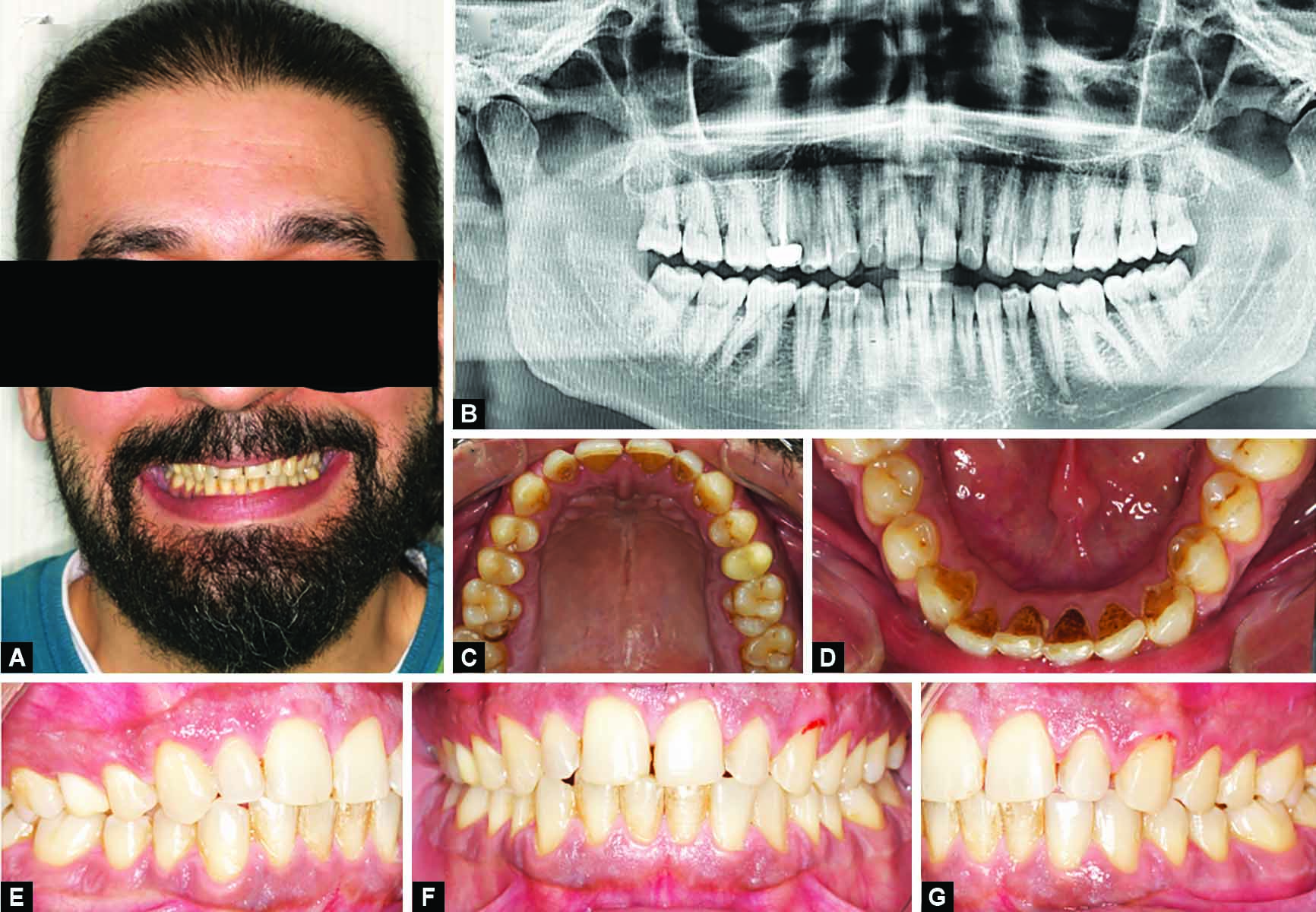
Figs 1A to G: Patient preoperative photos: (A) Smile view showing unproportioned dentition that is resistant to vital bleaching; (B) Preoperative panoramic radiograph; (C) Upper occlusal view photo; (D) Lower occlusal view photo; (E) Right lateral photo at maximal intercuspation; (F) Frontal retracted photo at maximal intercuspation; (G) Left lateral photo at maximal intercuspation
After the complete patient examination, 3Shape Software (3Shape Unite, Copenhagen, Denmark) was used to perform a two-dimensional smile design by inserting the different templates from the digital library into the patient’s extraoral photographs and communicating the results with the patient to understand the patient’s desire and expectations. The extraoral photographs (Figs 1A and 2A) were combined with intraoral scans (Fig. 2B) to 3D design the patient smile and create a virtual mock-up (Fig. 3) using the 3Shape Dental System. Two models obtained from the virtual mock-up were 3D printed using resin materials, one to be used as a clinical mock-up and the other to be used as a provisional model (Figs 4A, 5A and B).

Figs 2A and B: Retracted preoperative photo with the maxillary/mandibular intraoral digital scans screenshots from 3Shape viewer to be used for 3D digital smile design and virtual mock-up creation

Fig. 3: 3D digital smile design using 3Shape software

Figs 4A to C: 3D virtual mock-up using 3Shape software: (A) Frontal view showing the virtual mock-ups; (B) Clinical mock-up to 3D printed for patient motivation and guided tooth preparation for veneers; (C) Virtual provisional model to be 3D printed and fabrication of temporary veneers

Figs 5A to E: Frontal smile view of the patient with chairside esthetic try-in
A negative impression of the clinical mock-up model was obtained using PVS putty materials. Any tooth structure outside the outline of the virtual mock-up was maintained in this model to be able to seat the putty index with bisacrylate materials fully. The model for the clinical mock-up (Fig. 4B) was 3D printed to be used for patient motivation and guided tooth preparation for veneers. After that, any tooth structure extruded from the outline of the virtual mock-up was removed digitally, and the provisional model (Fig. 4C) was 3D printed for the fabrication of the chairside preparation guide using PVS putty materials and temporary veneers. For chairside preparation guide, the putty index was sectioned in multiple layers, buccolingually, mesiodistally, and cervico-incisally, to be able to check the amount of tooth reduction in relation to the form of the mock-up.
Veneer preparations were performed on the top of the guide using a bur with three guiding marks of 0.5 mm thickness and a chamfer finish line of 0.5 mm, and a butt joint 1.0 mm incisal preparation was performed.
Provisional veneers were fabricated chairside using “spot-etch technique,” where 37% phosphoric acid was applied as a spot on the central area of the facial surface of veneer preparation for 20 seconds, then rinsed and dried. Universal adhesive (3M™ RelyX™, St. Paul, USA) was applied at the etched spot and light cured for 20 seconds according to the manufacturer’s instructions. Bisacrylic material (Integrity, Dentsply Sirona, Charlotte, USA) was used to fabricate one-piece provisional veneers from maxillary right to left second premolars. Excessive materials were removed and the provisional prosthesis was finished, and polished.
Two retraction cords were used, sizes 00 and 0. Retraction cords were inserted into the gingival sulcus for 5 minutes. The retraction cord size 0 was removed, and an intraoral scan was performed for veneers #15 and #25 (Fig. 5C). The margin was defined digitally, and a high definition was obtained at the margins. The STL files were digitally transferred to a lab technician. Model 2 was used to fabricate provisional veneers that were cemented using the spot-etch technique.
The final laminate veneers were fabricated using CAD/CAM lithium disilicate (e.max CAD Low Translucency, Gurugram, India) shade A2 blocks with LT. Veneers were bonded to the tooth structure using resin cement (3M™ RelyX™, St. Paul USA) veneers cement “translucent” following the manufacturer’s instructions (Fig. 6). A follow-up examination was performed at 6 months and 1 year.

Figs 6A and B: Postveneer insertion and bonding: (A) Social smile; (B) Extreme smile while closing eyes
DISCUSSION
This article illustrated the use of digital technology in esthetic veneer cases. The digital veneer workflow starts with 3D digital smile design and virtual mock-up designing, 3D printing of the virtual mock-ups to motivate the patient to accept the treatment, and a chairside preparation guide to conserving as much enamel as possible during preparation. Treatment was initiated by obtaining digital diagnostic setups by incorporating digital scans and photography in a digital software (3Shape, Dental System, Denmark) to perform smile design and virtual mock-up, then translating it to the patient’s teeth using a putting index and autopolymerizing bisacrylic material (Integrity, Dentsply, Caulk). Using computer software to create diagnostic setups was advantageous in terms of saving time, particularly when modification of the diagnostic setup of one or more teeth in full-arch rehabilitation was required. This technique allowed us to precisely measure the reduction required for tooth-supported restorations to fulfill the esthetic and dental material requirements.1,2
The 3D printed mock-up was also used as a provisional mock-up for temporizing the preparations while the final veneers were under manufacturing. The digital setup was also used to design the final veneer restoration by superimposing the intraoral scan of the provisional veneers on the preparation scan and designing the final veneer prostheses accordingly. Thus, the predictability of the final treatment outcome was guaranteed to be similar to that of the patient approved at the initial stage of treatment.9
This digital workflow facilitated patient acceptance during the treatment planning discussion with the patient. Superimposing the full-arch esthetic try-in on the patient’s smile photo allowed the patient to visualize how his teeth would look after treatment completion. Using the digital setup to guide veneer tooth preparation resulted in a conservative reduction of the teeth, which protected their vitality and integrity.8
The intraoral digital scan yielded 3D images of tooth-supported preparations with high accuracy and resolution. Allows designing the final veneer protheses digitally without the need to digitize a conventional impression. Digital dentistry offers a predictable workflow to achieve precision in esthetic veneer cases and to enhance communication between the clinician, patient, and laboratory technician for efficient and optimal patient care.9,10,12
ACKNOWLEDGMENT
We want to thank Mr. Ibrahim Badran at 70 Digital Laboratory, Jeddah, Saudi Arabia, for performing the dental laboratory steps.
ORCID
Walaa Magdy Ahmed https://orcid.org/0000-0003-1810-8733
REFERENCES
1. Luo T, Li J, Xie C, et al. Accuracy of three digital waxing-guided trial restoration protocols for controlling the depths of tooth preparation for ceramic veneers. J Prosthet Dent 2022. DOI: 10.1016/j.prosdent.2021.12.029
2. Meereis CT, de Souza GB, Albino LG, et al. Digital smile design for computer-assisted esthetic rehabilitation: two-year follow-up. Oper Dent 2016;41(1):E13–E22. DOI: 10.2341/14-350-S
3. Okuda W. Smile design 1.0: learning from our past to meet the current challenge for predictable success. Gen Dent 2015;63(4):16–18. PMID:26147161.
4. Ortensi L, Sigari G, La Rosa GRM, et al. Digital planning of composite customized veneers using digital smile design: evaluation of its accuracy and manufacturing. Clin Exp Dent Res 2022;8(2):537–543. DOI: 10.1002/cre2.570
5. Qureshi T. The new age of ethical cosmetic dentistry: implementing the concept of progressive smile design. Dent Today 2012;31(10):98–101. PMID: 23156635.
6. Rebba B, Merlone A, Cantile N, et al. Digital smile planning technique applied to prosthetic rehabilitation of dental esthetic area: a case report. J Biol Regul Homeost Agents 2021;35(4 Suppl 1):1–9. DOI: 10.23812/21-4supp1-1
7. Sanchez-Lara A, Chochlidakis KM, Lampraki E, et al. Comprehensive digital approach with the digital smile system: a clinical report. J Prosthet Dent 2019;121(6):871–875. DOI: 10.1016/j.prosdent.2018.10.012
8. Stanley M, Paz AG, Miguel I, et al. Fully digital workflow, integrating dental scan, smile design and CAD-CAM: case report. BMC Oral Health 2018;18(1):134. DOI: 10.1186/s12903-018-0597-0
9. Trushkowsky R, Arias DM, David S. Digital smile design concept delineates the final potential result of crown lengthening and porcelain veneers to correct a gummy smile. Int J Esthet Dent 2016;11(3):338–354. PMID: 27433549.
10. Cattoni F, Mastrangelo F, Gherlone EF, et al. A new total digital smile planning technique (3D-DSP) to fabricate CAD-CAM mockups for esthetic crowns and veneers. Int J Dent 2016;2016:6282587. DOI: 10.1155/2016/6282587
11. Cattoni F, Tete G, Calloni AM, et al. Milled versus moulded mock-ups based on the superimposition of 3D meshes from digital oral impressions: a comparative in vitro study in the aesthetic area. BMC Oral Health 2019;19(1):230. DOI: 10.1186/s12903-019-0922-2
12. Ahlholm P, Sipila K, Vallittu P, et al. Digital versus conventional impressions in fixed prosthodontics: a review. J Prosthodont 2018;27(1):35–41. DOI: 10.1111/jopr.12527
13. Kong L, Li Y, Liu Z. Digital versus conventional full-arch impressions in linear and 3D accuracy: a systematic review and meta-analysis of in vivo studies. Clin Oral Investig 2022;26(9):5625–5642. DOI: 10.1007/s00784-022-04607-6
14. Ahmed WM, Hans A, Verhaeghe TV, et al. Managing excessive gingival display using a digital workflow. J Prosthodont 2020;29(5):443–447. DOI: 10.1111/jopr.13181
15. Chen X, Zhou N, Ding M, et al. A digital guiding device to facilitate cementation of porcelain laminate veneers. J Prosthet Dent 2020;124(4):411–415. DOI: 10.1016/j.prosdent.2019.10.011
________________________
© The Author(s). 2022 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted use, distribution, and non-commercial reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.