ORIGINAL ARTICLE | https://doi.org/10.5005/jp-journals-10019-1231 |
Impact of Overdried Preparation and Thermocycling on the Fracture of CAD–CAM Hybrid Ceramic Occlusal Veneer Restorations
1,4Department of Prosthodontics, College of Dentistry, University of Tennessee Health Science Center, Memphis, Tennessee, USA
2Department of Bioscience Research, College of Dentistry, University of Tennessee Health Science Center, Memphis, Tennessee, USA
3Department of General Dentistry, College of Dentistry, University of Tennessee Health Science Center, Memphis, Tennessee, USA
Corresponding Author: Antheunis Versluis, Department of Bioscience Research, College of Dentistry, University of Tennessee Health Science Center, Memphis, Tennessee, USA, Phone: +1 901 448 6372, e-mail: antheun@uthsc.edu
How to cite this article Edgerley PD, Versluis A, et al. Impact of Overdried Preparation and Thermocycling on the Fracture of CAD–CAM Hybrid Ceramic Occlusal Veneer Restorations. Int J Prosthodont Restor Dent 2019;9(2):38–42.
Source of support: We would like to thank Vita Zahnfabrik H. Rauter GmbH and Co. KG (Bad Sackingen, Germany) for their generous donation of the Vita Enamic blocks, and Innovative Dental Technologies Lab (Memphis, TN), specifically Darrin Throndson CDT and Josh Throndson CDT, for their time and laboratory resources in the fabrication of the occlusal veneers
Conflict of interest: None
ABSTRACT
Aim: To study the impact of overdried preparations prior to cementation with a self-adhesive resin cement and thermocycling on the fracture of hybrid ceramic occlusal veneer restorations.
Materials and methods: Sixty extracted maxillary molars were mounted and sectioned to remove the coronal structure 4 mm above the cementoenamel junction, leaving a flat area of exposed dentin and peripheral enamel. Ultrathin occlusal veneers with 0.3 mm central fossa thickness were milled from CAD–CAM hybrid ceramic (Vita Enamic). Teeth were randomly divided into three groups. After a selective enamel etching with phosphoric acid, groups I and II were blot-dried using cotton pellets; group III was desiccated with pressurized air for 15 seconds prior to cementation with a self-adhesive resin cement (Rely-X Unicem). Groups II and III were thermocycled between 5/55°C for 5000 cycles. The restored teeth were loaded axially until fracture. Fracture patterns were classified as fracture in the veneers only or fracture involving the tooth structure.
Results: The fracture strengths (mean ± standard deviation) were 1672 ± 585, 1789 ± 722, and 1586 ± 711 N for groups I (control), II (thermocycled), and III (overdried and thermocycled), respectively. No statistically significant differences were indicated (one-way ANOVA, p = 0.6426). Fracture patterns were significantly different (the Kruskal–Wallis rank sum test for multiple independent samples, p = 0.01315, followed by the Dunn post hoc test), where group III had more fractures in the veneer only than groups I and II.
Conclusion: Thermocycling of samples and overdrying of preparations did not show a significant difference in failure strength. However, fracture patterns indicated more veneer-only fractures under desiccated conditions, suggesting compromised restoration bonding.
Keywords: Fracture, Laboratory research, Occlusal veneers, Self-adhesive resin cement, Strength, Thermocycling.
INTRODUCTION
Tooth wear is a common condition seen in the dental practice.1,2 Diet, medical condition, and oral habits all can lead to abrasion, attrition, and erosion of the enamel and dentin. This loss of tooth structure can cause a variety of dental sequelae for patients, including occlusal disharmonies, musculoskeletal disorders, esthetic concerns, and the overall poor dental satisfaction.3 When treating patients with severe dental wear, alteration of the occlusal vertical dimension is frequently indicated. Increasing occlusal vertical dimension typically requires restoration of multiple teeth on both arches in order to arrive at an appropriate occlusion. This can be difficult and costly to the patients, as finding an appropriate occlusal vertical dimension typically requires multidisciplinary restoration of multiple teeth and trial periods to successfully arrive at an ideal functional state.4,5
In the interest of preserving the tooth structure and limiting elective devitalization or a periodontal surgery, minimally invasive dental preparations and restorations have become a common trend in dentistry and have proved beneficial to patients undergoing extensive fixed prosthodontic therapy.6 One such restoration modality, occlusal veneers, have been studied and shown to be a reversible and affordable means of increasing occlusal vertical dimension, allowing staging of complex treatment for severe tooth wear.7–10 Studies have shown that ultrathin occlusal veneers can withstand axial loads higher than typical human masticatory forces.7,8,11,12 Specifically, ultrathin occlusal veneers made from a hybrid ceramic material (Vita Enamic, VITA Zahnfabrik H. Rauter GmbH and Co. KG, Bad Säckingen, Germany) showed a fracture strength comparable to that of CAD–CAM composites.8 Vita Enamic is made by infiltrating polymer materials (urethane dimethacrylate, triethylene glycol dimethacrylate) into a porous ceramic network (Vita Enamic Technical and Scientific Documentation). Studies showed that it has mechanical properties that fall in between those of resin composites and ceramics and a microstructure similar to a natural tooth.13–15
Rely-X Unicem (3M, St Paul, MN, USA) is widely used as a self-adhesive dual cure resin cement and was used in similar studies of occlusal veneer fracture strength.7,8 Water is formed during the polymerization reaction of Rely-X Unicem, contributing to its hydrophilicity, moisture tolerance, and adaptation to moist dental surfaces.16 Wet dentin surfaces compromise adhesive strength.17,18 Overdrying of dentin prior to cementation, partly due to the habit of a thorough drying required by traditional luting agents, is however a common mistake when using a self-adhesive resin cement. The manufacturer of Rely-X Unicem instructs using cotton to dry off the preparation to avoid overdrying, but many clinicians and auxiliaries use an air syringe as a means of drying preparations. Studies indicate that overdrying can impact adhesive strength,19,20 but its effect on fracture strength has not been tested to our knowledge.
In the present study, in vitro failure strengths of an optimally bonded ultrathin Vita Enamic occlusal veneer was compared with a bonding protocol in which the veneer was cemented to an overdried preparation. Previous studies have shown that thermocycling, a means of artificial aging, decreases the bond strength of restorations to the dentin and enamel, possibly by water diffusing into the interfacial spaces, as can be expected during an intraoral use.21–23 Therefore the effect of thermocycling on the failure strengths of the occlusal veneers was also tested. The main purpose of this study was to investigate whether overdried cementation protocol of the self-etched resin cement and thermocycling affects the fracture strength of Vita Enamic occlusal veneer restorations. The null hypothesis was that overdrying and thermocycling would not significantly affect the failure strength and fracture characteristics.
MATERIALS AND METHODS
Tooth Preparation
Sixty extracted human maxillary molars with similar dimensions (mesio-distal dimension: 9.67 ± 0.68 mm; bucco-lingual dimension: 11.18 ± 0.73 mm) were collected and stored in distilled water. The unidentified teeth had been collected from dental practices, where they had been extracted for periodontal reasons or as wisdom teeth, and would have been discarded. The collection and use of these extracted teeth in our study was approved by the Institutional Review Board of the University of Tennessee Health Science Center (IRB# 17-05332-NHSR). The teeth were thoroughly debrided of the soft tissue and mounted in an auto-polymerizing acrylic resin (SamplKwick, Buehler, Lake Bluff, IL, USA) 4 mm apical to the cement-enamel junction (CEJ) and stored in distilled water. The coronal structure of the teeth was removed 4 mm occlusal to the CEJ using a diamond saw (Isomet Plus Precision Saw, Buehler) cutting straight across. This left a flat area of the exposed dentin and peripheral enamel, simulating a clinical situation of severe tooth wear (Fig. 1). Indexing notches were placed on mesial and distal finish lines with a high-speed hand-piece and a round-ended rotary bur with irrigation (#ZR 850 FG.01, Komet, Rock Hill, SC, USA). Teeth were visually examined and discarded if any existing cracks or pulpal exposures were present.
Restoration Design and Occlusal Veneer Fabrication
Preparations were scanned using a Trios 3Shape scanner (3Shape A/S, Copenhagen, Denmark). The acquired stereolithography (STL) files were exported to a professional dental laboratory. Occlusal veneers were designed to have the same occlusal anatomy using a cataloged maxillary molar tooth form and to have a central fossa thickness of 0.3 mm, while maintaining marginal adaptation to the individual tooth preparation. The occlusal veneers were milled from computer-aided design/computer-aided manufacturing (CAD/CAM) hybrid ceramic (Vita Enamic) blocks. Following milling, sprues were trimmed using a high-speed diamond bur (#ZR 850 FG.01, Komet) and the final veneers were checked for any defects in fabrication and marginal fit. Veneers that did not show adequate marginal fit and margins detectable with an explorer were discarded.

Fig. 1: Mounted teeth and preparation for occlusal veneer
Cementation
The inner surfaces of the milled Vita Enamic restorations were abraded with 50 μm aluminum oxide at 1.8 bar of pressure (Basic Quatro 230/240, Renfert GmbH, Hilzingen, Germany), cleaned with alcohol, and dried with oil-free pressurized air from a dental unit. The mounted teeth were randomly divided into three groups of 20 prior to cementation. A sample size of 20 had a 95% confidence to detect a difference of 0.4 standard deviations between the groups. The first and second groups (I and II) were to be bonded optimally, while the third group (III) would be overdried prior to bonding. Selective enamel etching was performed because Rely-X Unicem studies have shown that phosphoric acid etching of the enamel has a positive effect on adhesion of the cement, whereas etching of the dentin affects the bonding negatively owing to the self-adhesive cement’s inability to infiltrate collagen depleted by the etching.17 Therefore, only the enamel was etched with 37.5% phosphoric acid (Total Etch, Ultradent, South Jordan, UT, USA) for 15 seconds. Preparations were rinsed and blot dried with cotton pellets to avoid desiccation in groups I and II. The preparations in group III were dried with an air syringe at 10 cm from the dentin at the center of the preparation for 15 seconds until the dentin was completely dried, reproducing a clinically overdried preparation. All samples were cemented using the Rely-X Unicem (3M ESPE, St Paul, MN, USA) universal self-adhesive resin cement. A pressure of 6 N was used to seat the veneer, using a custom-fabricated seating device, and the residual cement was removed. Light polymerization (Valo cordless curing light, Ultradent) was performed for 20 seconds on buccal, lingual, mesial, and distal surfaces. All samples were stored in distilled water following cementation.
Thermocycling
Samples in group I were stored in distilled water at room temperature with no additional interventions. Samples from groups II and III were thermocycled between 5°C and 55°C for 5,000 cycles. Restorations were kept hydrated in distilled water at room temperature until they were tested.
Failure Load
After seven days of storage, the restored teeth were placed in a universal testing machine (Series 5567, Instron Co, Norwood, MA, USA) and subjected to an increasing occlusal load until fracture under displacement control at a crosshead rate of 0.5 mm/minute. Loads were recorded by a 10 kN load cell. The load was applied with a rounded (7 mm diameter) stainless-steel tip that simulated an opposing cusp (Fig. 2). The rounded tip was positioned to achieve tripodization of contacts along the cuspal inclines over the central fossa. The restored teeth were axially loaded along their long-axis, perpendicular to the prepared surface. The failure load in Newton (N) was the highest recorded load value before an at least 25% drop in load was observed. Failure strengths were statistically analyzed using one-way analysis of variance (ANOVA) at a significance level of 0.05.
Failure Pattern
Fracture surfaces were inspected and photographed under a stereomicroscope with a digital camera (SZX16 and UC30, Olympus, Tokyo, Japan). Failure patterns were classified as involving the veneer only or involving both the veneer and the tooth structure (enamel and/or dentin). The counts of each failure pattern for each group were subjected to a nonparametric Kruskal–Wallis rank sum test for multiple independent samples at 0.05 significance level, followed by Dunn test post hoc comparison with adjusted p value by Benjamini–Hochberg FDR method.
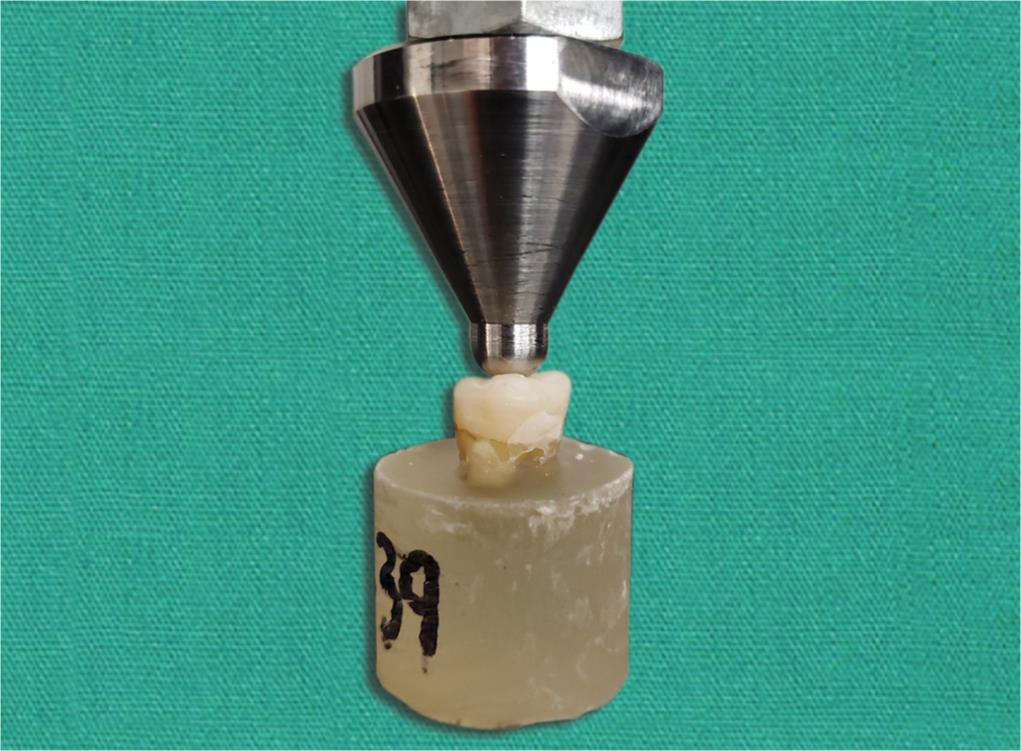
Fig. 2: Mounted teeth restored with ultrathin occlusal veneers under axial loading in a universal testing machine
RESULTS
Mean failure loads and fracture patterns for each group are listed in Table 1. One sample in group III was lost during the experimental phase. No statistically significant differences were found between the three groups (one-way ANOVA, p = 0.6426). Groups I and II suffered most failures that involved the tooth, while group III had the highest occurrence of failures that only involved the veneer. Examples of fracture patterns are shown in Figure 3. A significant difference in fracture pattern was detected among the three groups (Kruskal–Wallis rank sum test, p = 0.0132). The Dunn test post hoc test indicated that the fracture pattern of group III (overdried and thermocycled) was significantly different from groups I (optimal bond, no thermocycling) and II (optimal bond, thermocycled) with p values 0.0108 and 0.0457, respectively. Groups I and II were not significantly different (p = 0.4101).
DISCUSSION
The null hypothesis that challenging the bond would not show a significant difference in failure strength was accepted. No statistically significant differences were found in the failure loads of the ultrathin occlusal veneers when their preparations had been overdried during precementation procedures or aged by thermocycling. However, overdrying the preparation did cause significant differences in fracture patterns.
Bond strength is an important consideration for restoration retention and recovery of structural integrity. Overdrying and thermocycling are generally expected to reduce bond strength.21–24 However, this study did not measure bond strengths, but instead the structural strength of an ultrathin veneer in combination with the restored tooth under a specific clinically relevant load application. Therefore, the measured failure loads tested the implication of bonding for the fracture behavior of occlusal veneers rather than the bonding between the veneer and tooth on its own.
Occlusal veneers are typically used in situations where patients are undergoing significant occlusal reconstruction and thus will have their occlusion clinically managed with centric and excursive contacts carefully designed through thorough diagnostics.25 Considering the occlusal anatomy of our occlusal veneers, axial loading down the central fossa of the tooth was performed to simulate closure during mastication and clenching.26 Under such axial loading conditions, failure loads are likely more determined by the thickness of the occlusal veneers than by the bonding conditions, which may explain why failure loads were not significantly affected by overdrying or thermocycling. Observed variation in failure loads was probably mainly caused by the small anatomical variations in tooth size and properties. Efforts were made to use teeth that were similar in size. In addition, all veneers were designed to have the same occlusal anatomy, the same central fossa thickness, and underwent the same precementation treatment of their intaglio surfaces. Yet, natural variation in morphology and properties of the tooth structure may have played a role in bonding and fracture behavior, and it can be argued that the variations in failure loads represent clinical reality.
| Failure load (N) | Fracture involves veneer only | Fracture involves veneer and tooth structure | |
|---|---|---|---|
| Optimally bonded (group I) | 1672 ± 585 | 1 | 19 |
| Optimally bonded and thermocycled (group II) | 1789 ± 722 | 3 | 17 |
| Overdried preparation and thermocycled (group III) | 1586 ± 711 | 8 | 11 |

Figs 3A and B: Examples of fracture patterns: (A) Fracture only involves veneer; (B) Fracture involves both the veneer and the tooth structure (enamel or enamel and dentin)
Whereas overdrying or thermocycling did not significantly affect failure loads, a significant difference in the fracture pattern was indicated for samples in which the preparation had been overdried. It can be expected that a restoration with poor bonding is more likely to fracture without taking off tooth structure, as the cement would be the weakest link. On the other hand, strong bonds would be more prone to take tooth structure with it when structural failure occurs. A post-fracture inspection of the veneer-only fractures frequently showed remaining cement present on both the tooth structure and the veneer, indicating failure in the cement.27 The same observation was reported in a previous study.8 On the basis of this consideration, our study supports the notion that bonding under optimal manufacturer-recommended conditions provides a better bond than when overdried, since groups I and II had significantly less veneer-only failures than group III. A report that Rely-X Unicem exhibited higher bond strengths when dentin was not overdried lends further support to this explanation.19 Although optimal bonding resulted in more clinically destructive fractures involving the tooth structure, such catastrophic failures tended to occur far above the typical 585–880 N human masticatory forces.26,28
Challenging the bond with thermocycling did not cause significant differences in fracture modes. A thermocycling regimen of 5,000 cycles was used for this study. This number of cycles is estimated to represent 6–12 months of aging under clinical conditions,29,30 which is a reasonable period for a provisional restoration. Although a longer thermocycling regimen eventually may have led to changes in fracture patterns, our current results seem to corroborate another study that reported that thermocycling had no effect on the bond strength of the Rely-X Unicem.24 To the best of our knowledge, there are no long-term studies yet on the efficacy of Vita Enamic occlusal veneers as definitive restorations. However, the in vitro failure loads attained in this study are in agreement with other studies that concluded that occlusal veneers fabricated from the Vita Enamic could be a viable and economic treatment option for patients needing to increase the vertical dimension as a provisional measure and beyond.8,9
Some inherent limitations were present in the study. In vitro tests cannot replicate all clinical conditions. For example, some studies have noted an impact of pulpal moisture during cementation on bond strength.18 With this being an in vitro study using extracted teeth, it did not include this aspect. Moreover, the flat restored tooth surface was a simplification of severely worn surfaces, and did not feature thin peripheral enamel and reparative dentin frequently found in clinical cases.
The axial compressive loading may also be construed as an over-simplification of human clenching and mastication. The cusp height was designed to be clinically relevant for restoring worn dentition and was kept relatively short with a shallow fossa to simulate the restoration of a patient with severe wear.31 This was also done to ensure that much of the force would be transmitted to the tooth as a vertical compressive force, similar to previous relevant studies.7–9 A rounded spherical load tip was used to simulate an opposing cusp. Owing to the tripodization of contact between this tip and occlusal anatomy, forces were not purely vertical compression. This simulated a clinically relevant situation, as occlusal forces are rarely purely vertical.26,28 Off-axial and lateral loading to simulate bruxism could be addressed by a future study. The present study supports the use of ultrathin ceramic hybrid veneers as provisional restorations of severely worn teeth. Clinicians should be aware that overdrying the preparation could affect the bond quality of self-adhesive resin cement.
CONCLUSION
Within the limitations of this in vitro study, the following conclusions can be made:
- There were no statistically significant differences in the failure load of teeth restored with Vita Enamic ultrathin occlusal veneers when cementation was challenged by overdrying the preparation or thermocycling.
- Overdrying caused a significant change in fracture pattern, showing more restoration-only fractures, indicating compromised bonding.
ACKNOWLEDGMENTS
This study was part of a master of dental science research project. We would like to thank Cindy Deaton CDT and Mr Brian Morrow for their assistance in this study.
REFERENCES
1. Abrahamsen TC. The worn dentition - pathognomonic patterns of abrasion and erosion. Int Dent J 2005;55(4 Suppl 1):268–276. DOI: 10.1111/j.1875-595X.2005.tb00064.x.
2. Van’t Spijker A, Rodriguez JM, et al. Prevalence of tooth wear in adults. Int J Prosthodont 2009;22(1):35–42.
3. Turner KA, Missirlian DM. Restoration of the extremely worn dentition. J Prosthet Dent 1984;52(4):467–474. DOI: 10.1016/0022-3913(84)90326-3.
4. Hellsing G. Functional adaptation to changes in vertical dimension. J Prosthet Dent 1984;52(6):867–870. DOI: 10.1016/S0022-3913(84)90001-5.
5. Fayz F, Eslami A. Determination of occlusal vertical dimension: a literature review. J Prosthet Dent 1988;59(3):321–323. DOI: 10.1016/0022-3913(88)90182-5.
6. Edelhoff D, Liebermann A, et al. Minimally invasive treatment options in fixed prosthodontics. Quintessence Int 2016;47(3):207–216. DOI: 10.3290/j.qi.a35115.
7. Johnson AC, Versluis A, et al. Fracture strength of CAD/CAM composite and composite-ceramic occlusal veneers. J Prosthodont Res 2014;58(2):107–114. DOI: 10.1016/j.jpor.2014.01.001.
8. Egbert JS, Johnson AC, et al. Fracture strength of ultrathin occlusal veneer restorations made from CAD/CAM composite or hybrid ceramic materials. Oral Sci Int 2015;12(2):53–58. DOI: 10.1016/S1348-8643(15)00017-8.
9. Magne P, Stanley K, et al. Modeling of ultrathin occlusal veneers. Dent Mater 2012;28(7):777–782. DOI: 10.1016/j.dental.2012.04.002.
10. Angerame D, De Biasi M, et al. Influence of preparation designs on marginal adaptation and failure load of full-coverage occlusal veneers after thermomechanical aging simulation. J Esthet Restor Dent 2019;31(3):280–289. DOI: 10.1111/jerd.12457.
11. Al-Akhali M, Chaar MS, et al. Fracture resistance of ceramic and polymer-based occlusal veneer restorations. J Mech Behav Biomed Mater 2017;74:245–250. DOI: 10.1016/j.jmbbm.2017.06.013.
12. Ioannidis A, Mühlemann S, et al. Ultra-thin occlusal veneers bonded to enamel and made of ceramic or hybrid materials exhibit load-bearing capacities not different from conventional restorations. J Mech Behav Biomed Mater 2019;90:433–440. DOI: 10.1016/j.jmbbm.2018.09.041.
13. Coldea A, Swain MV, et al. Mechanical properties of polymer-infiltrated ceramic-network materials. Dent Mater 2013;29(4):419–426. DOI: 10.1016/j.dental.2013.01.002.
14. Della Bona A, Corazza PH, et al. Characterization of a polymer-infiltrated ceramic-network material. Dent Mater 2014;30(5):564–569. DOI: 10.1016/j.dental.2014.02.019.
15. He LH, Swain M. A novel polymer infiltrated ceramic dental material. Dent Mater 2011;27(6):527–534. DOI: 10.1016/j.dental.2011.02.002.
16. Radovic I, Monticelli F, et al. Self-adhesive resin cements: a literature review. J Adhes Dent 2008;10(4):251–258.
17. Yoon SY, Park SH, et al. Effect of dentin surface wetness on tensile bond strength of self-adhesive resin cements. J Korean Acad Conserv Dent 2009;34(2):113–119. DOI: 10.5395/JKACD.2009.34.2.113.
18. Mazzitelli C, Monticelli F, et al. Effect of simulated pulpal pressure on self-adhesive cements bonding to dentin. Dent Mater 2008;24(9):1156–1163. DOI: 10.1016/j.dental.2008.01.005.
19. Guarda GB, Gonalves LS, et al. Luting glass ceramic restorations using a self-adhesive resin cement under different dentin conditions. J Appl Oral Sci 2010;18(3):244–248. DOI: 10.1590/S1678-77572010000300008.
20. De Munck J, Vargas M, et al. Bonding of an auto-adhesive luting material to enamel and dentin. Dent Mater 2004;20(10):963–971. DOI: 10.1016/j.dental.2004.03.002.
21. Ehlers V, Kampf G, et al. Effect of thermocycling with or without 1 year of water storage on retentive strengths of luting cements for zirconia crowns. J Prosthet Dent 2015;113(6):609–615. DOI: 10.1016/j.prosdent.2014.12.001.
22. Blatz MB, Sadan A, et al. In vitro evaluation of shear bond strengths of resin to densely-sintered high-purity zirconium-oxide ceramic after long-term storage and thermal cycling. J Prosthet Dent 2004;91(4):356–362. DOI: 10.1016/j.prosdent.2004.02.001.
23. Wegner SM, Gerdes W, et al. Effect of different artificial aging conditions on ceramic-composite bond strength. Int J Prosthodont 2002;15(3):267–272.
24. Lüthy H, Loeffel O, et al. Effect of thermocycling on bond strength of luting cements to zirconia ceramic. Dent Mater 2006;22(2):195–200. DOI: 10.1016/j.dental.2005.04.016.
25. McHorris WH. Occlusal adjustment via selective cutting of natural teeth. J Gnathol 1997;16(1):37–51.
26. Koolstra JH, Van Eijden T, et al. A three-dimensional mathematical model of the human masticatory system predicting maximum possible bite forces. J Biomechanics 1988;21(7):563–576. DOI: 10.1016/0021-9290(88)90219-9.
27. Piwowarczyk A, Bender R, et al. Long-term bond between dual-polymerizing cementing agents and human hard dental tissue. Dent Mater 2007;23(2):211–217. DOI: 10.1016/j.dental.2006.01.012.
28. Kikuchi M, Korioth TWP, et al. The association among occlusal contacts, clenching effort, and bite force distribution in man. J Dent Res 1997;76(6):1316–1325. DOI: 10.1177/00220345970760061201.
29. Morresi A, D’Amario M, et al. Thermal cycling for restorative materials: Does a standardized protocol exist in laboratory testing? A literature review. J Mech Behav Biomed Mat 2014;29:295–308. DOI: 10.1016/j.jmbbm.2013.09.013.
30. Guidance on Testing of Adhesion to Tooth Structure. ISO/TR 11405 Dental Materials, International Standards Organization; 1994. pp. 1–14.
31. McHorris WH. Occlusion with particular emphasis on the functional and parafunctional role of anterior teeth. Part 2. J Clin Orthod 1979;13(10):684–701.
________________________
© The Author(s). 2019 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted use, distribution, and non-commercial reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.